Case Studies and Whitepapers
In the Era of Leukoreduction, are CMV-Seronegative Tested Blood Products Beneficial?
Transmission of cytomegalovirus (CMV) from blood transfusion can cause life-threatening infections in immunocompromised patients, including hematopoietic stem cell transplant recipients and neonates. CMV-associated pneumonia, hepatitis, and inflammation of the GI tract can lead to significant morbidity and mortality in these patients. Historically, CMV seronegative blood components have been the standard of care for protection from CMV acquired via transfusion. Blood products tested and found to be negative for IgG antibody against CMV are labeled as ‘CMV seronegative’. These products are actively used today to mitigate CMV disease risk but are in limited supply due to the high prevalence of CMV antibody in some blood donor populations.
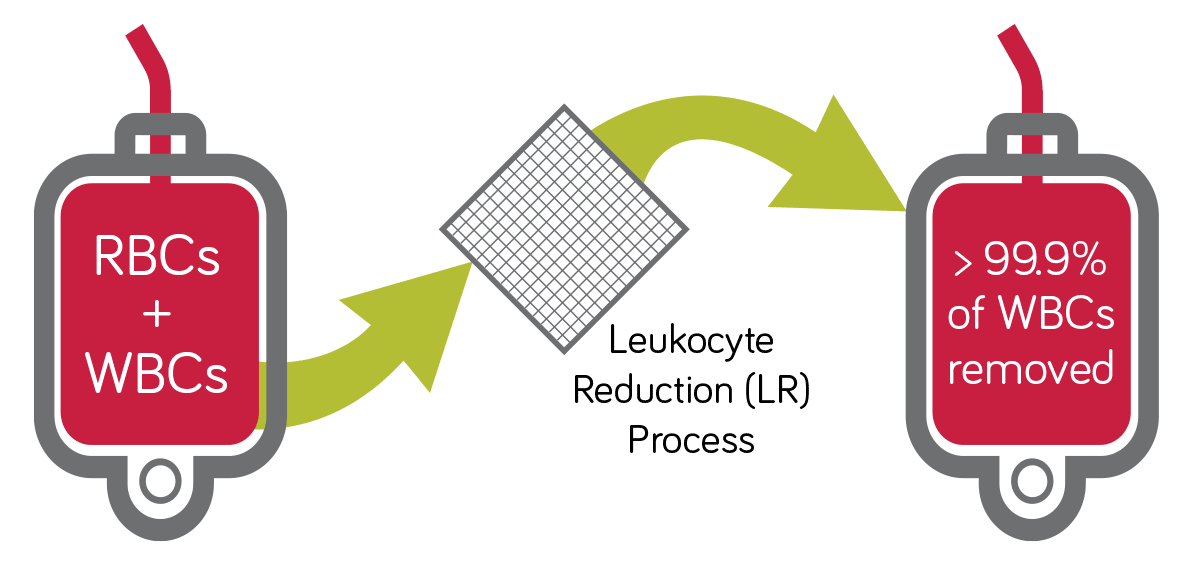
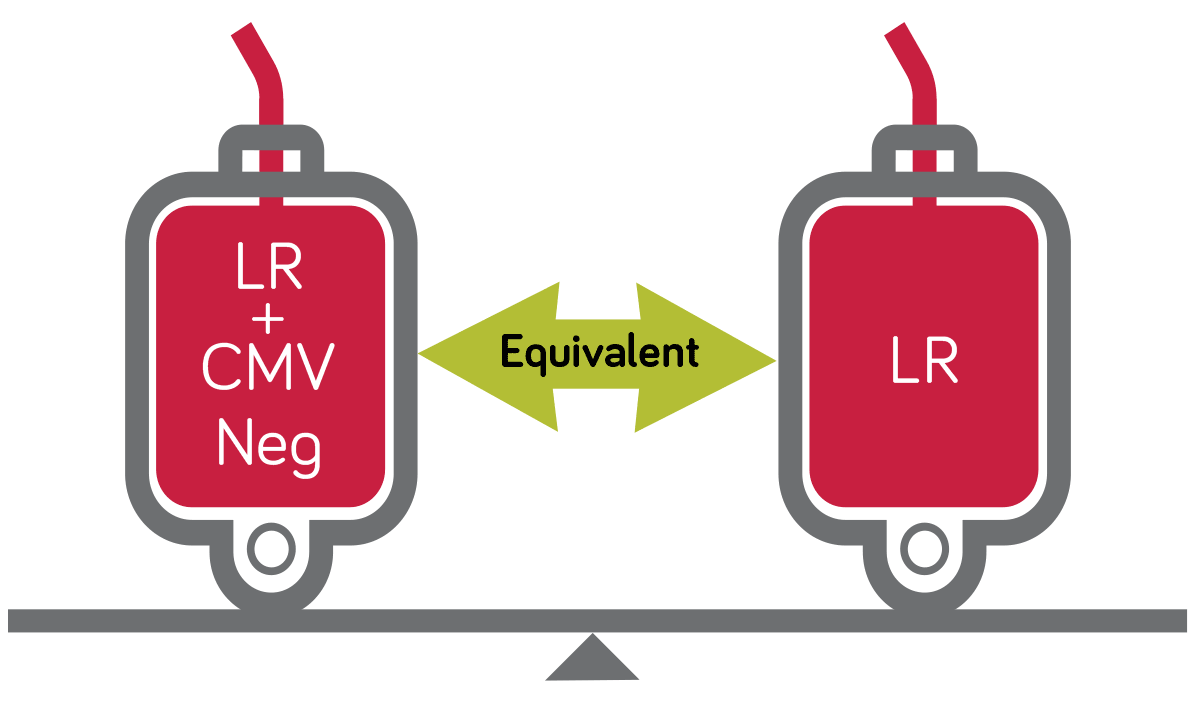
Leukoreduction (LR) of cellular blood products (red blood cells and platelets) also reduces the risk of transfusion-transmitted CMV (TT-CMV). LR efficiently removes white cells that harbor latent CMV virus. As a result, LR is widely considered equivalent to CMV seronegative tested products. Today in the US more than 90% of red blood cells and 95% of platelets transfused are pre-storage LR.1 In fact, a majority of US hospitals currently practice universal leukoreduction.2
The efficacy of CMV mitigation has been a hotly debated topic since the true transmission rate following transfusion is largely unknown and no strategy entirely eliminates the risk. Earlier studies on the prevention of TT-CMV disease in transfusion recipients involved blood products that were CMV seronegative or LR, but not both. In these studies either CMV seronegative tested blood or LR modification of the blood component was effective in reducing the risk of CMV infection.3
With the increasing use of pre-storage leukocytereduction and acceptance of universal leukoreduction, practices at some hospitals adapted to the use of CMV seronegative plus LR to fill orders for “CMV Negative” blood. A limited supply of certain blood components though has caused the transfusion community to question the added value of providing CMV seronegative blood products that are LR for the prevention of TT-CMV. This dogma of “dual strategy” for CMV prevention has been recently challenged in studies involving high risk patients.
Hematopoietic Stem Cell Transplant (HSCT) Patients
CMV seronegative transplant recipients receiving bone marrow or hematopoietic stem cells from a matched CMV negative donor (CMVneg/CMVneg) have the highest risk post-transplant for TT-CMV. In 1995, a prospective randomized control trial showed similar seroconversion rate for CMV antibody in allogeneic hematopoietic stem cell transplant (HSCT) patients whether transfused with LR only blood prepared by bedside filtration (a less effective method than current prestorage leukoreduction) or transfused with non-LR, CMV seronegative components.4 The study was underpowered, however, to definitively state which strategy was superior over the other for preventing severe CMV disease.
CMV seronegative blood remained the mainstay for mitigation of TT-CMV until a few years ago. Since 2011 several small retrospective observational studies.5,6,7 have shown that CMV seronegative tested RBCs and platelets that were also LR did not provide any additional benefit in preventing CMV infection in HSCT patients. These studies analyzed the incidence of CMV disease in over 400 high risk HSCT patients before and after changing the institution’s protocol from LR plus CMV seronegative blood products to LR only, CMV unscreened blood. HSCT patients were monitored for laboratory and clinical evidence of CMV viremia for up to 1 year post-transplant.
Cumulative results from two of the three studies demonstrated all patients to be negative for CMV NAT.5,6 In one study7 three patients in the LR, CMV seronegative group developed CMV viremia (CMV NAT positive) compared to only one patient in the LR only group. These findings contradicted the presumed superior safety for use of both LR and CMV seronegative products. Additionally, in 2015 Hall and colleagues reported no episodes of CMV infection in 76 high risk HSCT patients receiving LR, CMV unscreened blood components at two transplant centers in the UK.8 The results from these four recent studies, which include the transfusion of more than 9,000 LR, CMV unscreened blood components, support the practice of LR only blood for prevention of TT-CMV in HSCT patients.
Low Birth Weight Preterm Infants
CMV transmission in premature infants was previously attributed to blood transfusion but breastfeeding has now been found to be the most common transmission route.9 Many of the earlier studies evaluating postnatal TT-CMV in neonates were confounded by the CMV seropositivity of the mother. As high as 60% of mothers are seropositive for CMV, and in many of these mothers CMV DNA is present in expressed breast milk.9
Risk for TT-CMV infection is especially concerning in the very low birth weight (VLBW) or less than 1500 grams, premature neonates. As a prevention strategy for these neonates, LR plus CMV seronegative blood products is commonly used though the practice varies among hospitals in the US.10
The effectiveness of LR only versus LR plus CMV seronegative blood for preventing CMV infection in neonates has not been robustly studied. However, historical and recent pilot studies provide guidance.
A 1989 multicenter controlled study in Australia11 compared pre-storage LR blood to unfiltered blood for prevention of TT-CMV infection in VLBW neonates born to CMV negative mothers. There were no significant differences in gender, gestational age, birth weight, and number or volume of transfusions between the LR and unfiltered groups. All infants received some CMV seropositive blood and were followed for 6 months. In the LR cohort, none of the 30 infants became infected; whereas 9 of the 42 (21%) infants who received unfiltered blood developed CMV infection.
Likewise, a 2016 pilot study of 20 VLBW infants showed the overall incidence of TT-CMV to be 0% when using LR only blood products.12 Eight of the 20 infants received a total of 43 LR only blood transfusions of which 17 were from CMV seropositive donors. In comparison, zero incidence of TT-CMV was also found in 310 VLBW infants who were transfused with LR plus CMV seronegative blood components.9
While larger trials assigning neonates to CMV seronegative plus LR or LR only may help assess the best prevention measure for TT-CMV in neonates, such studies do not seem feasible given the low rates of infection. In addition, estimates for the probability of transmission of CMV in a pre-storage LR blood product are incredibly low, reported at 1 in 13.5 million.13 Therefore, since there is no current evidence that favors one strategy over the other for reducing the risk of TT-CMV in infants, it is generally believed and practiced that LR alone is adequate.
Recommendations
- Recent transplant center experience support the use of LR, CMV unscreened blood products in high-risk patients, particularly those receiving HSCT. No added benefit appears to exist for use of LR plus CMV seronegative blood products in preventing CMV infection in this patient population.
- While the evidence for use of LR only blood products in VLBW infants is limited, historical and recent studies suggest no clinical difference in outcomes for LR only versus LR plus CMV seronegative blood in this high risk group.
- Each transfusion service, in collaboration with their blood supplier and medical staff, should establish guidelines for use of LR only and/or LR plus CMV seronegative products for prevention of TT-CMV in high-risk patients. The current evidence presented here can serve as guidance to optimize the care for these at-risk patients while promoting more effective management of the blood supply.
Summary of Recommendations:
Equivalency of Leukoreduced (LR), CMV Negative versus LR, CMV Unscreened for Blood Selection in Specific Patient Populations
| Indications | LR + CMV Neg | LR, CMV Unscreened | |
| Allo CMV Neg HSCT pts/candidates | ✔ | ✔ | |
| CMV Neg solid organ transplant pts/candidates | ✔ | ✔ | |
| CMV Neg pts w/HIV | ✔ | ✔ | |
| CMV Neg pregnant female | ✔ | ✔ | |
| VLBW Neonates | ✔ | Likely |
References:
- Rajbhandary S, Whitaker BI, Perez GE. The 2014-2015 AABB Blood Collection and Utilization Survey Report. AABB 2018.
- Sapiano MRP, et al. Supplemental findings from the National Blood Collection and Utilization Surveys, 2013 and 2015. Transfusion 2017; 57:1599-1624.
- Vamvakas EC. Is white blood cell reduction equivalent to antibody screening in preventing transmission of cytomegalovirus by transfusion? A review of the literature and meta-analysis. Transfus Med Rev 2005;19(3):181-199.
- Bowden RA et al. A comparison of filtered leukocyte-reduced and cytomegalovirus (CMV) seronegative blood products for the prevention of transfusion-associated CMV infection after marrow transplant. Blood 1995; 86 (9):3598-3603.
- Nash T et al. Safety of leukoreduced, cytomegalovirus (CMV)-untested components in CMV-negative allogeneic human progenitor cell transplant recipients. Transfusion 2012; 52:2270-2272.
- Thiele T et al. Transmission of cytomegalovirus (CMV) infection by leukoreduced blood products not tested for CMV antibodies: a single center prospective study in high-risk patients undergoing allogeneic hematopoietic stem cell transplantation. Transfusion 2011; 52: 2620- 2626.
- Kekre N et al. Is cytomegalovirus testing of blood products still needed for hematopoietic stem cell transplant recipients in the era of universal leukoreduction? ASBMT 2013; 19:1719-1724.
- Hall S et al. Transfusion in CMV seronegative T-depleted allogeneic stem cell transplant recipients with CMV-unselected blood components results in zero CMV transmissions in the era of universal leukocyte reduction: a UK dual centre experience. Transf Med 2015; 25(6):418-423.
- Josephson C et al. Blood transfusion and breast milk transmission of cytomegalovirus in very low birth weight infants. JAMA Pediatrics 2014; 168(11); 1054-1062.
- Smith D, et al. Survey of current practice for prevention of transfusion transmitted cytomegalovirus in the United States: leucoreduction vs. cytomegalovirusseronegative. Vox Sanguinis 2010; 98:29-36.
- Gilbert GL, et al. Prevention of transfusionacquired cytomegalovirus infection in infants by blood filtration to remove leucocytes. Neonatal Cytomegalovirus Infection Study Group. Lancet 1989 Jun 3; 1(8649):1228- 1231.
- Delaney M, et al. Postnatal cytomegalovirus infection: a pilot comparative effectiveness study of transfusion safety using leukoreduced-only transfusion strategy. Transfusion 2016; 56:1945-50
- Seed CR, et al. The residual risk of transfusion-transmitted cytomegalovirus infection associated with leucodepleted blood components. Vox Sanguinis 2015; 109: 11–17.